Placebo and Opioid analgesia - imaging a shared neuronal network. This is the most difficult paper of the lot. I would read the abstract, intro, and the last few paragraphs, and skim the rest, unless you can follow the details of their experiments.
This article talks about an endogenous opioid system in the brain. The basic idea is this: Opioids like morphine, codeine, heroin obviously affect human pain (as well as other things). Hence they act as analgesics. How do these opioids work? As all other drugs, they must bind to “receptor” protein, probably located in neuron membranes. Why would these plant molecules bind to human neural protein receptors? Candice Perk had the idea that there must be “endogenous” opioid molecules in our own bodies, whose function is pain analgesia. These molecules have been found, and include endorphins (endogenous morphins), enkephalins, andanamide (the endogenous analog of THC, the active ingredient in marijuana). The exogenous and endogenous "opioids" bind to the same receptors.
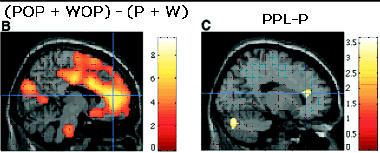
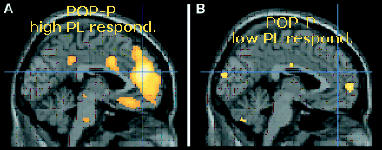
In this article, they look at brain activity in two regions of the brain (rostral anterior cingulated cortex – rACC) and the brainstem) that are known to be activated in the presence of opioids. For patients treated with opioids, they used the opioid remifentanil which was injected intravenously. PET (positron emission tomograph) scans of the brain were made. This scans look for increased neural activity in certain regions of the brain. When the exogenous opioid remifentanil (or endogenous opioid released in placebo responses) binds to the opioid receptors, neural activity increases in the area of opioid binding. Before injection of the drug, a special "isotopic" form of water (in which the oxygen atom has 7 neutrons in its nucleus instead of 8) is given to the subjects. This can be taken up in the brain and stimlulated to release gamma rays in activated neurons. These activated neurons are detected and used to generated the brain scans shown in the article.
POP: PAIN (HOT) + OPIOIDS
WOP: WARM + OPIOIDS
P: PAIN (HOT)
W: WARM
PPL: PAIN (HOT) + PLACEBO
P: PAIN
.
2. Expectation and Dopamine Release: Mechanism of the Placebo Effect in Parkinson's Disease - .
This is an easier read. In Parkinson's disease, neurons that release the neurotransmitter dopamine, are dying. Hence dopamine levels in certain parts of the brain decrease. Drug therapy includes L-DOPA, which is converted to dopamine in the brain. This study again used PET and the dopamine like drug, raclopride. It binds to the same receptor proteins on neurons that dopamine does. The more dopamine that is present, the less this drug binds. This drug has a carbon which has one fewer neutrons than normal, and like the example above, releases gamma rays. Parkinson symptoms have been known to be decreased by placebos. Do placebos increase the release of dopamine in the brain? Read the article
3. Placebo-induced changes in fMRI in the anticipation and experience of pain.
This paper is again quite complicated so I would focus on the intro and the concluding paragraphs. Try to get the main point of the article, without getting lost in the details. This paper uses functional magnetic resonance imaging (fMRI) to study changes in brain activity during analgesia. They note that placebos have been shown to decrease pain perception. This effects is diminished by a drug that binds to opioid receptors that blocks the activity of that receptor. Such drugs, such as naloxone, are called antagonist.
The also note the naloxone, independent of placebo, can produce hyperalgesia (a condition of altered perception such that stimuli which would normally induce a trivial discomfort cause significant pain). These effect could block any analgesia produced by a placebo. This study tries to differentiate possible mechanisms of the placebo effect.